I recently came across a news article on the disproportionately devastating impact of COVID19 pandemic on the victims of the Bhopal gas tragedy.1 This news motivated me to revisit and learn more about the event that happened over 35 years ago. The Bhopal gas leak tragedy is the world’s worst industrial disaster. Methyl iscocyanate (MIC), a compound used to manufacture pesticides, was released from the Union Carbide India Limited’s (UCIL) chemical factory located in the city of Bhopal, the capital of the Indian state of Madhya Pradesh. Then Danbury, Connecticut, United States (US) based Union Carbide Corporation (UCC) established the Mumbai based UCIL as its Indian subsidiary to manufacture and market pesticides in the country. The US corporation held majority shares of 50.9% and the rest of the shares were held by various Indian insurance companies, Indian banks, Indian government and Indian investors. The land where the company stood was leased from the Madhya Pradesh state government.
{kind=link}
The gas released during the Bhopal gas tragedy: MIC is a highly toxic and irritant chemical. Even at concentrations of 2ppm, it is extremely toxic to humans.2 This catastrophic event resulted in nearly 3800 deaths and over 500,000 injuries. The gas leak that happened over 3 decades ago still continues to have adverse health effects on the survivors of this tragedy. The chronic effects of MIC exposure are in the form of increased incidence of cancer, respiratory disease, reproductive disorders, greater number of stillbirths, higher than usual spontaneous abortions3 and now during the COVID19 pandemic, an increased risk of mortality among those victims. The survivors of the tragedy also suffers from various mental health issues including post traumatic stress disorder, from having to witness and experience the gassing to death of thousands and injuring even more individuals. It left unfathomably deep scars on the psyche of Bhopal and India. Even though the Bhopal gas tragedy happened before I was born, it was one of the dominating news events of my childhood during the 1990s. Even with the constant exposure about the Bhopal gas tragedy right from a very young age, after my recent research into the tragedy, I came across a few previously unknown facts that took me by great surprise.
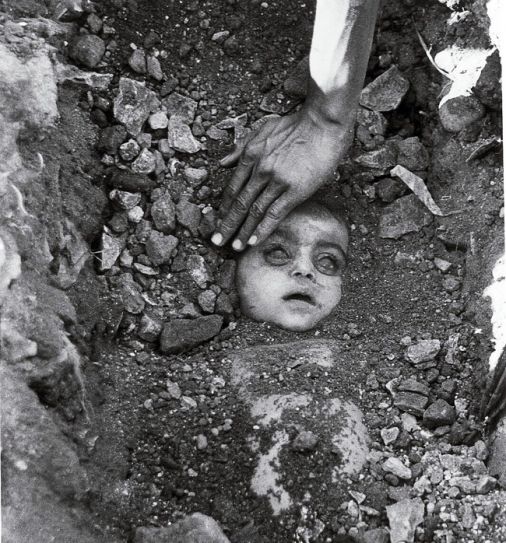
(Copyright disclaimer: Copyright belongs to the original copyright holder. This image is reproduced here under the provision for fair usage of copyright content for research and commentary purposes. )
The biggest surprise of all to me was the cause of the Bhopal gas leak. On 2nd December, 1984, the UCIL employees undertook an unreported, riskier, modified maintenance procedure, during the second shift (14:45 hours to 22:45 hours), around 21:30 hours. Water was injected through a pressure gauge tap near the MIC storage tank 610. This pressure gauge tap was located very close to the common valve located over the tank 610. This tap provided a more direct access to a malfunctioning diaphragm motor valve (DMV) that could not be cleaned properly using the routine water-washing maintenance procedure. The restoration of normal functionality of the DMV was critical for nitrogen pressurization and therefore the MIC transfer from tank 610. During this off-the-books operation by the UCIL employees, they inadvertently introduced 500kg of water into the MIC tank 610.4 This human error caused a massive heat releasing chemical reaction within the tank 610 that resulted in the Bhopal gas tragedy.
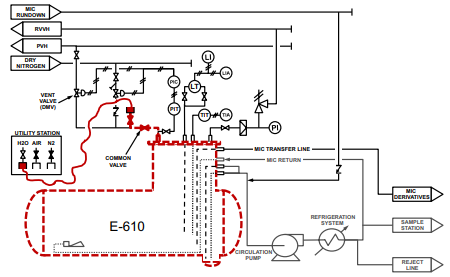
(Copyright disclaimer: Copyright belongs to the original copyright holder. This image is reproduced here under the provision for fair usage of copyright content for research and commentary purposes. )
Approximate timeline of events
| 2nd December 1984 |
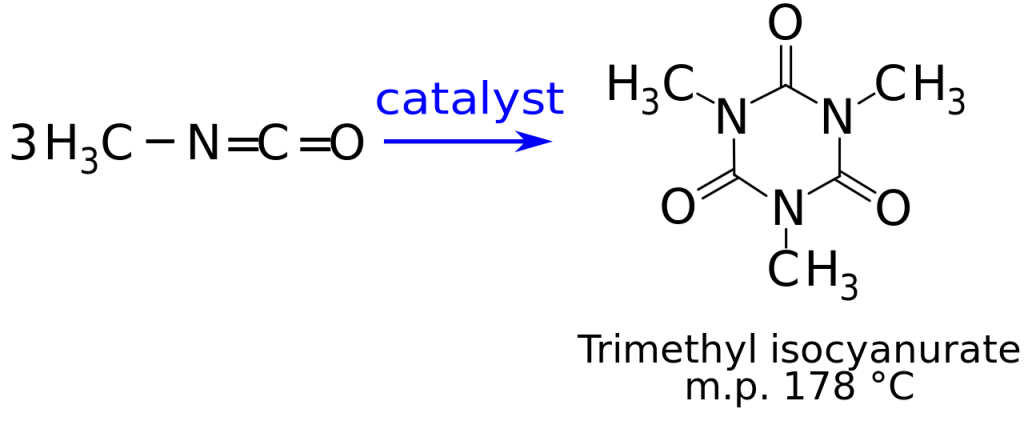
| Unknown period before 21:30 hours : The UCIL Bhopal plant manager and the MIC supervisor formulated a modified water-washing procedure that was supposed to establish a more direct water access route to a malfunctioning diaphragm motor valve (DMV) due to trimethyl isocyanurate crystal deposition. The role of UCC, the parent company of UCIL is unknown in the formulation of this modified maintenance plan. The modified water-washing plan involved removal of a pressure gauge closer to the common valve near the storage tank 610 and then inject water through the pressure gauge tap. The employees overseeing this modified maintenance plan sketched diagrams depicting how to inject water through the pressure gauge tap in their daily log book. But, most importantly, their planning did not account for the possibility of trimethyl isocyanurate crystal depositions on the common valve as well. 21:30 hours: The employees started the modified cleaning procedure for the DMV through the pressure gauge tap near the MIC storage tank 610. The workers established water pressure across the DMV. The workers performed a cursory check to see if the common valve was closed. The trimethyl isocyanurate crystal deposits blocking the common valve gave a false sense of security to the operators by offering feedback resistance to the valve closure attempts. In reality, the common valve was jammed open due to the trimethyl isocyanurate crystal deposits inside the valve body. Between 21:30 hours and 22:30 hours: Trimethyl isocyanurate crystal plug around the common valve dissolved away restoring the normal functionality of the common valve. It was therefore left in a partially open position. Since the modified water washing procedure was an unsupervised one, water started to pour into the MIC storage tank 610, with no one noticing it. Between 22:30 hours and 22:45 hours: Brief spikes in the pressure gauge readings for the tank 610 were noticed by the workers manning the gauges. The pressure increase was due to the release of the gaseous products during the heat producing reaction between MIC and water. The pressure rise was quickly nullified by the subsequent escape of those gases through the same route that was established for the modified water-washing procedure. The gases from the chemical reaction inside the tank escaping through the process valve header (PVH) resulted in the tearing effects around the MIC storage area. Between 22:45 hours and 23:00 hours: The workers looking for a leak detected a constant dripping of yellowish white substance near the process valve header (PVH), relief vent valve header (RVVH) area. This leak was due to the escaping of the gaseous products of the chemical reaction in the tank, through the modified water-washing route. If the modified water-washing process was working as expected, there should have been a steady flow of water from the PVH-RVVH area. Instead the reported leakage of yellowish fluid clearly indicated the escape of reaction products between MIC and water. The workers from the newly changed night shift noticed the water hose connected to the pressure gauge tap for the modified water-washing procedure, near the common valve of the MIC storage tank 610. They feared the worst and checked the common valve, which they found to be left in an open position. They quickly closed the common valve and disconnected the water hose. They also found that the water was still running through that hose at the time their discovery. 23:30 hours: The workers started reporting significant tearing effects around the MIC storage tank area. 23:45 hours: The workers investigating the leak in the MIC storage area reported to the MIC supervisor about the leak near the PVH-RVVH area. The MIC supervisor misunderstood the MIC leak for a water leak, because a water leak was the expected outcome from the modified maintenance process. Between 23:45 hours and 00:15 hours: With the common valve near the storage tank 610 properly closed, the tearing effect temporarily subsided. But, the pressure was building-up inside the tank 610, due to the auto-catalytic, exothermic reaction between ~500kg of water and 80 metric tonnes of MIC. |
| 3rd December 1984 |
| Between 00:15 hours and 00:30 hours: The usual late night tea service was noted to be unusually quiet and the mood was gloomy. The employees of the plant had realized that water had entered the storage tank 610 through the pressure gauge tap, during the modified maintenance operation. Between 00:30 hours and 00:40 hours: The pressure gauge recordings were steadily increasing. The pressure readings were inching closer to the operationally significant 40 psi level. The workers attempted to transfer the MIC in the storage tank to one of the transfer pots used for Sevin production, using the pressure build-up inside the storage tank. The amount of MIC transferred was insufficient to reduce the pressure build-up inside the storage tank. Between 00:40 hours and 00:45 hours: The temperature inside the storage tank exceeded 25 degree Celsius, the maximum recording range for the temperature gauge. The pressure of the tank exceeded 40 psi, resulting in the breaking of the rupture disc, a safety device that was supposed to break when the pressure reached 40 psi. The safety valve in the next check point had also popped open. The concrete covering the tanks had cracked open. The chemical vapors from the reaction inside the tank along with the vaporized MIC started shooting out of the vents. 00:45 hours: The internal pressure of the storage tank 610 exceeded 55 psi. The MIC supervisor ordered shutting off all the water sources around the MIC storage area. The workers attempted to break down the MIC by spraying water on the toxic white cloud hanging over the storage area. But, the water pressure was insufficient to reach the height of the white cloud of leaked toxic gases. 00:50 hours: Vent gas scrubber (VGS), a system that was designed to inject caustic soda solution to breakdown the escaping gases was turned on. The meter showing caustic soda circulation indicated that there was none circulating inside the VGS. The VGS system failed to contain any of the gases escaping from the storage tank 610. 01:30 hours: The toxic white MIC cloud started engulfing the employee area. The employees started to panic. They ran away from the white cloud of death. Some of the employees had access to oxygen masks. They wore those oxygen masks and moved to safer downwind areas. 02:00 hours: The winds blew the toxic white MIC cloud slowly away from the factory site and it started its slow travel towards the city. It was just the beginning of the gassing to death of the Bhopal residents. After 02:00 hours: Once the chemical reaction subsided, since the common valve was inadvertently restored to its normal functionality during the modified maintenance procedure at around 21:30 hours on December 2nd 1984 and it was securely closed during the tank inspection around 22:45 hours on December 2nd 1984, the tank 610 managed to retain an absolute internal pressure of 3 psi, (~12 psi below atmospheric pressure) for nearly 20 days. This was a surprising vindication for the designers of the storage system, that their design could withstand an explosive decompression. But, that robust storage system alone was clearly demonstrated to be insufficient in preventing a catastrophic gas leak. 06:00 hours: The senior instrumentation supervisor arrived early to inspect the storage tank 610. He discovered that a pressure gauge was missing from the storage tank 610 area and a hose with water still running out of it, right next to the pressure gauge tap. |

The purpose of the modified water-washing maintenance procedure was to establish a more direct water access line to the diaphragm motor valve (DMV) that led to the process valve header (PVH). This valve malfunctioned due to trimethyl isocyanurate (MIC trimer) crystal deposition. The faulty valve prevented the nitrogen pressurization of the tank to transfer out the stored MIC. After the MIC production was terminated in October, two attempts to pressurize the tank 610 using nitrogen, the first one on 30th November, 1984 during the first shift (06:45 hours to 14:45 hours) and the second one on 1st December, 1984 during the second shift (14:45 hours to 22:45 hours), were unsuccessful. The employees were working against a literal ticking clock to fix the malfunctioning valves. Time was running out for the once promising pesticide manufacturing plant in Bhopal. The investors and the parent corporation had run out of patience and decided to shut down the plant, dismantle everything and ship it off either to Brazil or Indonesia.6 The industrial manufacturing license from the Madhya Pradesh government was going to expire on 1st January, 1985. The parent company Union Carbide Corporation was going to withdraw from the Indian partnership.
The employees were left with only a handful of days to convert the stored MIC to a technical grade pesticide product at the nearby Sevin manufacturing facility. But, to accomplish that, they needed to first transfer the stored MIC from tank 610 to the 1 ton production pots used by the Sevin team. When the plant was new, the employees accomplished this using transfer pumps. But, once the transfer pumps started failing frequently, also due to the deposition of trimethyl isocyanurate crystals, the factory abandoned the transfer pumps altogether. They started to use the nitrogen pressurization of the storage tanks to push out the stored MIC. The nitrogen pressurization also started failing due to valve leaks. Therefore the only way forward for the employees was to address those valve leaks as quickly as possible so that they could restart the nitrogen pressurization of the MIC storage tanks.
{kind=link}
In the minds of the employees that undertook this slightly revised operation, restoring the normal function of DMV was highly necessary to have a fighting chance to keep the plant operational. This covert maintenance procedure was very similar to a routine water-washing operation to clean the relief vent valve header (RVVH) and the process valve header (PVH). It could be the reason for initial reports that attributed the accident to a routine maintenance operation going wrong, but, could not explain the later insistence by the Indian government that the maintenance procedure was nothing but routine. But everyone involved in that process missed a key fact. Both the common valve and the DMV were made of iron. This made both those valves equally prone to the trimethyl isocyanurate crystal deposition. These crystal deposits often give a false feeling of security to plant operators managing the affected valves. For the untrained eye, the feed back resistance to the force that is applied to close the valve gives the impression of a securely shut-off valve. In reality the crystals are just blocking the valves from operating normally.
Critically, the employees overseeing the operation did not insert a blind to reduce the reliance on the common valve integrity. Even though this was mandated by the operation procedures and a safer method to accomplish an otherwise risky task, it would have increased the amount of work to perform an operation that they thought was routine and urgent. Also, since the plant was seriously understaffed due to several brutal cost-cutting exercises, waiting for an overburdened maintenance staff to come around and install a valve blind would have further delayed their ability to transfer MIC for Sevin production. Time was of essence for the remaining UCIL staff in Bhopal, even if that meant taking a few extra risks here and there. This covert maintenance operation was probably also an attempt by the employees to demonstrate their value to the management, so that, even if the Bhopal plant was shutdown, they had a fighting chance of being employed elsewhere in the large network of factories under the Union Carbide umbrella.

Initially everything proceeded normally. Sadly, it was the proverbial calm before the storm. Despite this cleaning attempt being clearly riskier and off-the-books, the employees tasked with this operation added another layer of risk by sticking with the usual method employed during routine water-washing maintenance operations. They let the water run uninterrupted for 3 hours, that too without any supervision. Once the water pressure was established across the DMV, the employees that undertook the cleaning operation left their shifts and handed the plant operations over to the employees of the next shift (22:45 hours to 06:45 hours). During this time, the trimethyl isocyanurate deposits in the common valve washed away. The common valve was in partially open position after all the crystal deposits were washed away. Since the water connection was closer to the common valve, the basic hydraulics dictated that the water would go directly through the common valve and into the MIC storage tank 610. Assuming that the water must have been leaking into the tank right from the start of that modified maintenance operation, the water entry continued for well over two hours. Approximately 500kg of water entered the storage tank during that time period. Even though MIC is a relatively stable chemical, mixing of water with MIC results in a powerful exothermic chemical reaction. Soon enough, the unintended entry of large amounts of water triggered a violent heat producing chemical reaction.
The stored MIC was already at room temperature, even before the modified water-washing operation started. The company recommended storage temperature for MIC was supposed to be at zero degree Celsius. But, due to an earlier cost-cutting decision to disconnect the refrigeration system, the MIC storage tanks were no longer maintained at a steady zero degree Celsius. This refrigeration system was also meant for MIC storage temperature control. Once the water started pouring-in, the resultant chemical reaction between MIC and water caused the temperature in the storage tank to rise quickly. With no temperature controlling mechanism in place, it soon exceeded the boiling point of MIC. This resulted in the conversion of the remaining un-reacted liquid MIC into its gaseous form.
Since the MIC tank was 80% full, the volume of the gases produced during the exothermic reaction could not be contained in the vessel. There was also no option of safe transfer of the boiling, violently reacting MIC to the other two storage tanks. The other two storage vessels also contained large quantities of MIC. The pumps designed to transfer the materials from the storage tank were decommissioned as part of the plant liquidation process. So, the employees had to resort to yet another riskier procedure of transferring the boiling MIC to the Sevin manufacturing vats using the pressure build-up due to the chemical reaction. They performed this risky transfer of a batch of MIC using that technique, but, the amount removed was grossly insufficient to reduce the pressure build-up inside the tank. The storage tank acted essentially as a giant chemical reaction pot, with the employees having left with no options to control that violent reaction.
Finally, the vaporized MIC and the exothermic chemical reaction products escaped through the safety release mechanism, once the internal pressure of the storage tank exceeded its design limits. This resulted in the release of approximately 40 metric tons of MIC into the atmosphere. The employees decided not to inform the police. There was an informal company policy in place that forced employees to not alert the local law enforcement in the event of a gas leak. The alarm for alerting the public of a gas leak was also disconnected. Even if the alarm was activated, there were no warnings to an outside observer. The toxic white cloud hung over the MIC storage tanks, like the pristine white robe of an angel of death, slowly traveling along the breeze towards a sleeping city, with the people deep in slumber, unaware of their imminent ghastly deaths awaiting them.
Immediately after the gas leak, the thin veil of secrecy around the covert maintenance operation started falling apart quickly. Next morning, a senior instrumentation supervisor at the plant found that the pressure gauge attached to the tank 610 was missing. The plant logs showed that the particular missing pressure gauge was present on November 30, 1984, two days before the tragedy. The same instrument supervisor also stated to the investigators that he also found a hose lying beside the tank man-head that morning, with water still running out of it.9 Even though this testimony was used by the Union Carbide Corporation to build a case of sabotage, they selectively ignored the evidences that pointed towards the elaborate planning that happened as part of the modified maintenance operation. The ‘independent’ investigation report noted that they recovered a sketch depicting water injection through the pressure gauge in a daily log.9 This sketch was noted to have been made prior to the incident. On the other hand, Indian government, through CBI resorted to extreme intimidation and interrogation tactics against this supervisor. They dubbed this interrogation and intimidation exercise as ‘lie detection’, to force this individual to change his testimony to suit the government narrative that the water-washing operation was nothing but a routine operation.10
The other surprising fact I learned was the repetitive nature of history, in this instance, the lethal combination of human error and a clueless corporation. Union Carbide Corporation was a legacy corporation with very poor understanding of their own chemical process. This observation is in sharp contrast to the health and safety report published by UCC after the tragedy. In that report, the author portrayed UCC as a safety conscious organization. He especially waxed poetically about his mother imbibing him the quality of not telling any lies. But, the facts related to the Bhopal tragedy told me a totally different story. The Union Carbide Corporation lied. The Union Carbide Corporation lied to the investors and the public about their depth of understanding of their own chemistry. They also lied about the problems they were having with the Bhopal plant. They also lied about the extend of their involvement in running the Bhopal plant. The running of UCIL by UCC could be characterized as hands-off style corporate management, with minuscule amount of direct communications between their US headquarters in Danbury and their Indian counterpart in Mumbai. But, the US company forcefully exerted a huge influence on how its Indian subsidiary was running their daily operations, at the very least, the directions of those.
The sabotage theory was first revealed by the UCC’s ‘independent’ investigations into the tragedy. To protect themselves against defamation law suits in the US, the firm decided to never officially name the ‘saboteur’. Officially publicly naming the ‘saboteur’ could have opened themselves to a series of defamation lawsuits by the named parties. So, instead they let the media and the former employees do the reveal through the various publications and the Indian court system.6,7The sabotage theory was never really taken seriously by the Indian public, but the US court system loved the ingenuity of their argument. The sabotage theory spread by UCC is the worst example of corporate gas-lighting and racism, that is so convincing that it has outlived the very individuals who had created this fantasy tale.
The theory behind the sabotage was that, a disgruntled employee decided to spoil the MIC batches by pumping water into the MIC storage tank. It is a simple and easy to understand theory. No understanding of valve mechanics or chemical crystal formations or basic human decency is required to digest the crap-shoot of a hollywoodesque fantasy manufactured by UCC. Like a brilliant movie script, it had very clear motives, a very clear victim and a very clear villain. According to UCC representatives and the ‘independent’ investigators hired by UCC, the real victim was their incredible safety conscious corporation that could never do anything wrong. The villain in their eyes was a lowly paid, disgruntled, individual of color, living in a third world country and harbored resentments against a capitalist multinational corporation for ruining their career prospects. This clearly mad theory of sabotage was often dismissed by the Indian mainstream media as a distraction tactic by the US corporation that held majority shares in UCIL at the time. The media called it a tactic by UCC to shift the blame of the industrial accident onto a lowly paid employee at the facility.8
On the other hand, the media and the Indian government threw their weights around the notion that a routine maintenance procedure was responsible for this tragedy. The official communications around the Bhopal gas tragedy highlighted a flaw in the plant design which resulted in the water entering the MIC tanks during a routine water-washing maintenance operation that occurred a few hours before the tragedy.11 Even though the theory sounded plausible, the experts from the government and the ones hired by UCC who evaluated the plant design and ran various tests, accurately concluded that the routine maintenance operation of water-washing the process valve header (PVH) and the relief valve vent header (RVVH) lines could not have resulted in the entry of 500kg of water into the storage tanks.

During one of the federal investigations by the Indian government into the tragedy, the Indian Central Bureau of Investigations (CBI) and the Council for Scientific and Industrial Research (CSIR) investigators found no traces of water in the pipes that were supposed to have carried these large quantities of water into the MIC storage tanks, during a nitrogen purge. The investigators and the factory employees overseeing the purge were expecting gallons of water accumulated inside the plumbings that led to the MIC storage tanks. Following the nitrogen purge, they waited with large vats to collect the accumulated water. Instead, the pipes turned out to be bone-dry.9Even though this investigative exercise was never reported in the Indian media, this little known fact delivered a death blow to the most widely circulated theory in India for the Bhopal gas leak tragedy. For the routine water-washing maintenance gone wrong theory to be true, the water should have accumulated in some of the pipes that led to the MIC storage tanks. The absence of any water in these pipes conclusively proved that the some of the safety designs of the plant worked as expected.
The basic hydraulics confounded another easy to explain, but, totally flawed theory. The relatively low water pressure in the hoses used for cleaning combined with the drains being opened, ensured that the water would flow through those drains and not against pressure of a closed valve. The back pressure exerted against these valves would not be significant enough to result in water entering those tanks. The impossibility of water entering the MIC tanks through just a valve leak during a routine PVH-RVVH line cleaning was confirmed by both the independent experts hired by UCC9 as well during a follow-up investigation by the Indian federal investigators during the evaluation of the associated valves to see whether a valve failure could result in the water flow into the MIC storage tanks. These investigations could not demonstrate water accumulation in the MIC storage tanks.
The official CSIR report released in 1985, a year after the tragedy, had no mention of any obvious functional defects with the valve responsible for preventing the water entry into the MIC tanks during the pipe cleaning process. In retrospect, this was obvious because the common valve was inadvertently restored to its normal functional state, during the fateful modified maintenance operation. They also failed to report any obvious obstructions with the drains, which could have resulted in the build-up of water pressure. Even though the CSIR report agreed with the independent investigators that the MIC release was due to the entry of large quantities (~500kg) of water into the tank 610, they failed to provide a reasonable explanation for the presence of such large quantities of water.
The other supporting fact for the off-the-books cleaning operation and its effectiveness was the relative ease with which the MIC storage tank 610 held lower tank pressure than the atmosphere following the explosion. The CSIR investigators working to understand the causes of the MIC release noted on December 20th, 1984, that the tank 610 was maintaining an internal absolute pressure of 160mm Hg (~3 psi) and decided to increase the tank pressure to atmospheric levels using nitrogen.12 If the common valve was left in a partially open position due to the deposition of trimethyl isocyanurate crystals, the tank 610 would have been unable to maintain a negative internal pressure. In that case, at the time of inspection, the internal pressure of the tank 610 would have been equal to that of the atmospheric pressure. The tank 610 maintaining a significantly lower internal pressure than the atmosphere was another indirect evidence that the modified maintenance procedure resulted in the common valve being accidentally restored to its normal functional state. Therefore, the maintenance of a negative pressure and the subsequent nitrogen pressurization back to atmospheric levels were easy tasks to achieve within the storage tank 610. The fatal maintenance operation was in some ways a success in that, the tank 610 no longer had any leaks that previously plagued it.
The Bhopal gas leak was certainly neither a sabotage nor a routine water-washing maintenance operation gone wrong. The leading root causes promoted by both UCC and Indian federal government were total fabrications and falsehoods. Both parties were extremely reluctant in revealing the real cause of the release of large quantities of MIC in Bhopal.6,7Based on my research, the immediate cause behind the Bhopal gas tragedy was that: a group of employees’ last ditch efforts to keep a dying factory alive resulted in the release of large quantities of a lethal gas into the atmosphere of a city that was clearly unprepared for it.
The real truth behind the Bhopal tragedy was darker and even more complex than the simple explanations floated by both UCC and the Indian government. Like the inventive and imaginative lawyers hired by UCC, the Bhopal gas tragedy could be interpreted as a case of sabotage. But, the sabotage was not committed by a single employee. Union Carbide Corporation, its Indian subsidiary, the Indian bureaucracy and the investors of UCIL, all acted together in this sabotage process. Through a process of constant dilution of safety, misguided attempts at short-term cost cutting, enforcement of a culture that subjected employees to unnecessary risks without providing proper training and a toxic blame driven work culture, all combined forces to cause the tragedy that unfolded in Bhopal, over 35 years ago. The tragedy was definitely not because a smart, Indian mathematics graduate who was denied a meaningless promotion, showed-up for work on time and decided to spoil a batch of precious materials that were necessary to support his livelihood.
The question of how it happened is an easy answer and it is as follows: on 2nd December, 1984, a group of UCIL workers, while attempting to restore the functionality of the 610 MIC storage tank, resorted to desperation. The question of why it happened is more complex question to answer. The employees were simply trying to clean a valve that was rendered inoperable by the constant gremlin of trimethyl isocyanurate crystal formations. These crystals showed up everywhere in the MIC manufacturing plant, frequently interfered with the normal operation of the plant and were the proverbial nail in the coffin for the Bhopal plant. Yet, the management and the investors of UCIL tried to soldier-on without any meaningful mitigation efforts.
The insurmountable trimethyl isocyanurate crystal deposition problem was a direct consequence of the management’s miscalculated cost cutting efforts. Instead of addressing the root cause plaguing the production facility, the UCIL management forced the workers to work harder, denied promotions and burdened them with unknown and unacceptable risks. The nickels and dimes first, people last attempts to keep a dying industrial beast alive was definitely a megalomaniac and ill-informed exercise. It was doomed to fail from the start. The employees were deliberately set-up for failure by the UCIL management. The investors, the company and its parent corporation were ruthlessly trying to recoup every nickel and dime worth of their investments that was sunk into a failed plant, through shameless exploitation of their own employees. The employees were patiently tolerating this cruel corporate tyranny in the hopes of protecting their meager livelihoods. Out of sheer desperation the workers attempted a poorly thought-out, unscientific and extremely risky maintenance operation.
Unknown to every single one of them was the fact that, the water intended to wash away the gremlins and restart the pesticide production, also dissolved away the very crystals that were jamming the common valve leading to the 610 storage tank. Once the crystals dissolved away, the malfunctioning valves were restored to their normal functional state. That unfortunately meant, the common valve would be set in a partially opened position. There were no monitoring mechanisms for the water-washing process. There were no reliable temperature monitoring protocols implemented to detect any anomalous exothermal reactions occurring in the MIC storage tank. Soon, the free flowing water surged past the common valve and flowed directly into the tank brimming with a substance that was ready to react violently with water.
Before anyone had noticed this mistake, large quantities of water already entered the storage tank. After that gross miscalculation, it dawned upon those employees that nothing could stop the violent chemical reaction that was going to follow. Hence the reason for an eerily silence and an overarching gloomy mood that was reported by the immigrant tea vendor from Nepal during the routine late night tea service that happened around 12:15am, the morning of 3rd December 1984.9
After 35 years of lengthy court battles and untold amount of sufferings endured by the victims and their relatives, the haze of the tragedy is slowly subsiding and the facts are finally becoming more visible. Those facts are as ugly as the tragedy itself. The corporate falsehoods by Union Carbide Corporation was not very surprising. But, as a citizen of India, a great nation with its motto ‘let truth prevail’, I am genuinely appalled and ashamed that the erstwhile Indian administration would shamelessly lie and promote falsehoods to hide their own culpability in the worst industrial disaster.
2 https://pubchem.ncbi.nlm.nih.gov/compound/Methyl-isocyanate#section=Health-Hazards
3 https://www.atsdr.cdc.gov/MMG/MMG.asp?id=628&tid=84#bookmark02
4 Bloch, Kenneth. Rethinking Bhopal: a Definitive Guide to Investigating, Preventing, and Learning from Industrial Disasters. Elsevier, 2016. Print.
5Madhava, Menon N. R. Documents and Court Opinions on Bhopal Gas Leak Disaster Case: For Course on Tort-Ii (industrial and Mass Torts). Bangalore: National Law School of Indian University, 1991. Print.
9 http://storage.dow.com.edgesuite.net/dow.com/Bhopal/casestdy.pdf
10Union of India versus Union Carbide Corporation, Court of district judge, Bhopal, GAS CLAIM Case No. 1113, filed in 1986, decided on 3rd April 1987
11 https://www.nytimes.com/1985/01/28/world/the-bhopal-disaster-how-it-happened.html
12 “Report on Scientific Studies on the Release Factors Related to Bhopal Toxic Gas Leakage”, Indian Council of Scientific and Industrial Research, December 1985.